
History: Blau Syndrome, also known as familial juvenile systemic granulomatosis, is a hereditary (inheritable) autoinflammatory disorder named after the doctor who first documented it in 1985, Edward Blau. The disease is very rare and is prevalent in no more than one in a million people. It is mainly seen in Caucasian people.
:max_bytes(150000):strip_icc()/autoinflammatory-diseases-5084129_final-bd224608f04548d19017a6abced380d6.gif)
Causes: The disease is caused by the NOD2 gene on the 16q12 chromosome. Its inheritance is autosomal dominant. This means the disease is passed down if just one of the parents has the gene mutation that causes the condition. The NOD2 gene encodes the NOD2 protein, which activates an inflammatory response when interacting with bacteria. When a person has Blau syndrome, mutations in the protein lead to the overaction of inflammation in the entire body, even without a (bacterial) trigger.


Symptoms: Blau syndrome typically shows up in childhood. The three typical features are skin, joint, and eye-related. A skin rash is typically the first sign a person has the disease, within the first year of life. The second sign is arthritis which causes permanently bent fingers, usually from two to four years. The third sign is eye disease, which includes redness, pain, sensitivity to light, blurred vision, cataracts, and a reduction in eyesight. Some patients develop fevers and inflammation of the organs or the circulatory system. Inflammation of the organs can cause an enlarged liver, lung disease, and kidney disease. Inflammation of the circulatory system can cause hypertension (high blood pressure) and inflammation of the heart artery.

Diagnosis: A diagnosis can be hard to get, but once Blau syndrome is suspected, there are diagnostic procedures to utilize. These include genetic testing to identify a NOD2 mutation, a biopsy to identify immune cells, and imaging or X-rays. Another possible diagnosis other than Blau Syndrome is early-onset sarcoidosis (EOS), which shares many of the same characteristics. Other possible diagnoses include arthritis, Yao syndrome, sarcoidosis, lupus, vasculitis, tuberculosis, Lyme disease, syphilis, and Behcet’s disease.

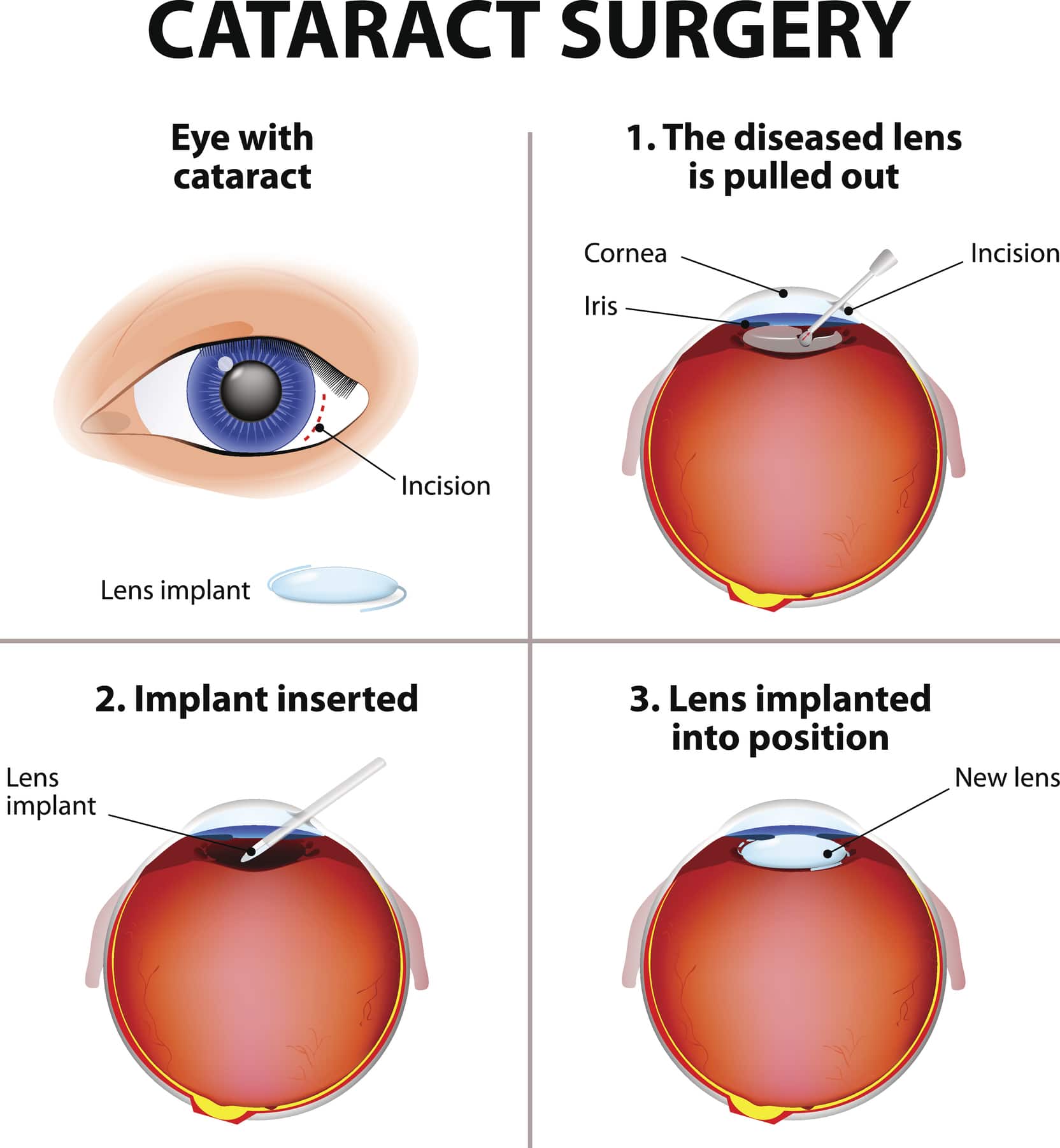
Treatments: There is no way to prevent Blau Syndrome, but genetic counseling can inform families that their future child could have it, thus getting an earlier diagnosis and treatment. Management of the disorder includes taking medications and having surgery. The recommended medical therapies are anti-inflammatory drugs, immunomodulatory drugs, immunosuppressants, or steroids. Although, there is no formal guidance for the treatment of the disease. A potential medical treatment is monoclonal antibody therapy, which utilizes synthesized proteins that act as antibodies. This is the same therapy used to treat COVID-19, however, for the treatment of Blau Syndrome, there is little evidence of its effectiveness. Surgery, such as arthrodesis (surgical fusion of the joint) or cataract surgery, is sometimes needed.

References
Blau, E. B. (1985). Familial granulomatous arthritis, iritis, and rash. The Journal of Pediatrics, 107(5), 689–693. https://doi.org/10.1016/S0022-3476(85)80394-2
Caso, F., Galozzi, P., Costa, L., Sfriso, P., Cantarini, L., & Punzi, L. (2015). Autoinflammatory granulomatous diseases: From Blau syndrome and early-onset sarcoidosis to NOD2-mediated disease and Crohn’s disease. RMD Open, 1(1), e000097. https://doi.org/10.1136/rmdopen-2015-000097
Kaufman, K. P., & Becker, M. L. (2021). Distinguishing Blau Syndrome from Systemic Sarcoidosis. Current Allergy and Asthma Reports, 21(2), 10. https://doi.org/10.1007/s11882-021-00991-3
Matsuda, T., Kambe, N., Takimoto-Ito, R., Ueki, Y., Nakamizo, S., Saito, M. K., Takei, S., & Kanazawa, N. (2022). Potential Benefits of TNF Targeting Therapy in Blau Syndrome, a NOD2-Associated Systemic Autoinflammatory Granulomatosis. Frontiers in Immunology, 13, 895765. https://doi.org/10.3389/fimmu.2022.895765
Matsuda, T., Kambe, N., Ueki, Y., Kanazawa, N., Izawa, K., Honda, Y., Kawakami, A., Takei, S., Tonomura, K., Inoue, M., Kobayashi, H., Okafuji, I., Sakurai, Y., Kato, N., Maruyama, Y., Inoue, Y., Otsubo, Y., Makino, T., Okada, S., … Nishikomori, R. (2020). Clinical characteristics and treatment of 50 cases of Blau syndrome in Japan confirmed by genetic analysis of the NOD2 mutation. Annals of the Rheumatic Diseases, 79(11), 1492–1499. https://doi.org/10.1136/annrheumdis-2020-217320
Miceli-Richard, C., Lesage, S., Rybojad, M., Prieur, A. M., Manouvrier-Hanu, S., Häfner, R., Chamaillard, M., Zouali, H., Thomas, G., & Hugot, J. P. (2001). CARD15 mutations in Blau syndrome. Nature Genetics, 29(1), 19–20. https://doi.org/10.1038/ng720
Yi Yong, C., Mukhtyar, C., & Armon, K. (2018). 65. Blau syndrome treated with sequential biologics. Rheumatology Advances in Practice, 2(suppl_1), rky034.028. https://doi.org/10.1093/rap/rky034.028

Leave a comment